Nearly one in every eight adults enrolled in Medicaid has a substance abuse disorder (SUD),[1] and a significant barrier to treatment is a shortage of SUD professionals[2] in every state. In response, state Medicaid agencies are developing and deploying a growing workforce of non-licensed, non-master’s-level treatment and support providers – such as peers, counselors, and other qualified staff – to provide a range of services to supplement licensed SUD provider capacity.[3] To help states address SUD workforce challenges and identify cutting-edge solutions, the National Academy for State Health Policy (NASHP) conducted a comprehensive review of how each state Medicaid program was paying for and overseeing non-licensed SUD staff. This brief summarizes what steps states are taking to reduce workforce shortages and provides resources to help states develop new approaches to expanding their SUD workforce.
How Medicaid Agencies Leverage their Non-Licensed SUD Workforce
To help states address SUD workforce challenges and identify cutting-edge solutions, NASHP conducted a comprehensive review of how each state Medicaid program was paying for and overseeing non-licensed SUD staff.
Background
NASHP analyzed publicly available materials to identify:
- How Medicaid agencies reimburse for SUD services provided by non-licensed, non-master’s-level workforce;
- What services they provide and in what settings; and
- State education, training, and supervision requirements for non-licensed staff.
NASHP used the most recently available Medicaid provider and billing manuals, state regulations, and other public policy documents (including state plans and waivers) for all 50 states and Washington, DC. Findings were grouped and coded to allow for easier cross-state analysis. The data collected was shared with Medicaid and other state leaders.
States’ non-licensed workforce was categorized as:
Peers: Individuals with lived experience providing Medicaid-billable SUD services.
Counselors: Individuals providing Medicaid-billable SUD counseling or therapy services without a state license.
Other Qualified Staff: Other non-licensed professionals providing Medicaid-billable SUD services who did not meet the definition of a “peer” or “counselor.”
Services funded by resources other than Medicaid (e.g., state grant funding) were considered outside the scope of this research.
The majority of state Medicaid agencies (42) reimburse for SUD treatment services provided by non-licensed, non-master’s-level SUD staff. NASHP’s scan identified 45 types of peers in 39 states, 52 types of counselors in 31 states, and 43 types of other qualified staff in 24 states. The services these staff may provide, where they provide the service and how they are reimbursed, as well as education, training, and supervision requirements all varied to some degree across states. Key findings are summarized below.
Service Delivery
State Medicaid programs pay for a range of services and supports delivered by non-licensed staff. These services were grouped in the following categories:
- Peer services;
- Screening, assessment, and evaluation;
- Brief intervention;
- Community and rehabilitative supports (e.g., education, skills training, and family support);
- Case management/care coordination; and
- Crisis intervention.
States reimburse counselors for a broad range of SUD services. In addition to counseling/therapy services, more than half of non-licensed counselors can be reimbursed by state Medicaid programs for screening, evaluation, assessment, community and rehabilitative support, case management/care coordination, and/or crisis intervention services. Most state Medicaid agencies pay peers to provide peer support services-only, although approximately one-quarter of peers may also be reimbursed to provide rehabilitative or supportive services. Other qualified staff generally fell into one of two groupings: individuals primarily providing case management or care coordination services or unlicensed staff providing rehabilitative or supportive services who did not meet state qualifications to provide counseling services.
States vary in the types of counseling/therapy services that may be provided by non-master’s-level counselors. For example, every state permits their non-master’s-level counselors to provide individual and/or group counseling services, but only two-thirds of states reimburse certified counselors for family counseling services. Florida only reimburses its bachelor’s-level counselors for group services, limiting reimbursement for individual and family services to those with a master’s degree.
Setting and Reimbursement
Non-licensed staff deliver services in licensed behavioral health agencies or facilities, typically working within a multidisciplinary care team. Although employed by licensed agencies or facilities, services may often be provided in home and/or community settings to meet the needs of individuals receiving treatment.
How services delivered by this workforce can vary, depending on whether services are provided in outpatient or residential settings. State Medicaid agencies commonly pay licensed behavioral health clinics for services delivered by non-licensed staff on a fee-for-service basis, through Current Procedural Technology or Healthcare Common Procedure Coding System codes that may include modifiers to designate provider type. In contrast, services delivered by non-licensed staff in intensive outpatient programs (including day treatment and partial hospitalization) or residential treatment programs tend to be reimbursed as part of a bundled, per-diem rate. States may also include these types of staff in bundled rates for specialty opioid treatment programs. For example, Maine, Michigan, and Rhode Island all include peers in their opioid health home programs.
Education, Training, and Supervision
Training for peers tends to be more individualized and state-specific. Most states require peers to complete an in-person training program (typically one to two weeks), often offered through a state health agency. Counselors, on the other hand, may receive training though approved courses offered by community colleges or other professional development programs. States generally rely on national exams for counselors but were more likely to use state-developed training and exams for peers. Whether the state’s board membership was with the National Association for Alcoholism and Drug Abuse Counselors (NAADAC) or the International Certification & Reciprocity Consortium (IC&RC) determined which national exam the state required for certification. Some states, particularly those with multiple credentialing boards, allow either exam.
Most states require that non-licensed, non-master’s-level SUD treatment staff be supervised by certified or licensed SUD providers, who often held a master’s degree. In many cases, state regulations identify multiple eligible providers who could supervise staff rather than requiring one specific provider type. For example, a bachelor’s-level counselor might be supervised by a psychiatrist, an advanced practice nurse with specialized addictions training, or a master’s-level counselor with supervisory training. It is also common for individuals, particularly for those without a counseling certification, to be supervised by a more experienced colleague holding a similar credential – for example, a peer with two years of experience would supervise another peer. States also routinely set minimum standards for the supervisory relationship, such as defining frequency of meetings and on-call availability. Positions requiring less training and experience typically required closer supervision. Clinical oversight requirements were generally less specific than supervisory requirements and sometimes vary by type of service. State Medicaid agencies generally require assessments and treatment plans to be signed/authorized by a physician, master’s-level provider, or nurse care manager.
Some state Medicaid programs offer and reimburse for trainee positions. Several states noted the importance of trainee programs in expanding their non-licensed staff capacity. Louisiana reimburses services provided by counselors-in-training, who are permitted to provide screening/evaluation/assessment services, counseling, and crisis intervention services under the supervision of a licensed mental health provider. Similarly, Washington State reimburses a chemical dependency professional trainee, who can provide screening/evaluation/assessment services, counseling, and case management/care coordination under the supervision of a certified individual who has completed some college.
Looking Forward
The number of state Medicaid agencies utilizing non-licensed, non-master’s-level SUD treatment staff is expected to increase in the coming years. Since 2015, the number of states using Section 1115 Medicaid Demonstration Waivers to augment or entirely transform their SUD treatment systems has grown significantly,[5] and many of these states now pay for services delivered by non-licensed staff.[4] The use of these and other relevant Medicaid authorities (e.g., the Medicaid rehabilitative services option or health home state plan option) to increase access to peers and other non-licensed SUD treatment professionals presents both opportunities and challenges for states.
- How to support best practices while recognizing state variability. Given the wide range of definitions and standards currently used by states, resources are needed for policymakers to better understand best practices, including where and how these non-licensed staff add the most value. While most non-licensed counselors need to pass a nationally recognized exam for certification, the roles permitted within diverse state Medicaid programs can be quite different. Similarly, training and examination requirements for peers and other qualified staff vary significantly from state to state. Sharing state resources on how non-licensed staff can support best clinical practices for SUD treatment and recovery may be helpful for future policy development.
- Ensuring cross-system collaboration to address co-occurring needs in integrated care Given the significant correlation between SUD diagnoses and co-occurring mental health and physical health conditions, appropriate training and use of non-licensed staff offers another opportunity for states to promote integrated care for high-cost, high-needs individuals. Moreover, as states increasingly look to health clinics and primary care providers to provide SUD and opioid use disorder (OUD) treatment, defining how these non-licensed staff can and should operate within those settings raises additional issues (and potential opportunities) for state policymakers to promote access to treatment and better integrate care.
- Supporting managed care: In states with managed care systems, important questions remain as to how plan-employed staff (particularly peer supports and care coordination/case management staff) can best work with their provider-level counterparts to efficiently and effectively meet the needs of individuals needing or receiving SUD treatment.
- How to integrate non-licensed staff in larger inpatient and residential facilities: Historically, the “Institutions for Mental Disease exclusion” has prevented states from paying for Medicaid services provided to adults ages 21 to 64 in behavioral health facilities with more than 16 beds. Recent federal guidance and programmatic changes have enabled state Medicaid agencies to pay for services for adults in these settings using Section 1115 waiver authority.[6] While models exist, how to incorporate non-licensed staff into these settings will likely be of significant interest for state policymakers going forward.
Conclusion
State Medicaid agencies are increasingly using non-licensed workforce – including counselors, peers, and other qualified staff – to meet the growing need for SUD treatment and recovery services by their Medicaid-enrolled populations. NASHP’s review of how states oversee and pay for these services highlights opportunities. Understanding key trends in oversight and payment for this staff will provide a baseline for states as they seek to leverage and expand this workforce. Additionally, the significant variability in how states use these staff, what services they provide, and the kinds of training, education, and supervision they receive speak to a larger need for additional resources for state policymakers to effectively utilize this valuable part of the SUD workforce.
Other Resources
State Medicaid agencies are increasingly leveraging non-licensed workforce, including peers, to meet the growing need for SUD treatment and recovery services by their Medicaid-enrolled populations. For an overview of cross-cutting themes and additional analyses of how states are paying for other non-licensed workforce, please refer to the following companion documents in this series:
- Key Findings from a 50-State Scan of State Medicaid Requirements for Non-Licensed SUD Workforce: Peers
- Key Findings from a 50-State Scan of Medicaid Requirements for Non-Licensed SUD Workforce: Counselors
- Key Findings from a 50-State Scan of Medicaid Requirements for Non-Licensed SUD Workforce:
Other Qualified Providers - Medicaid Reimbursement Categories Key for Non-Licensed SUD Workforce
State Medicaid Requirements for Peers
The National Academy for State Health Policy (NASHP) analyzed reports and regulations from all 50 states to identify how their Medicaid programs reimbursed for non-licensed, non-master’s-level substance use disorder (SUD) staff – including counselors, peers, and other qualified staff – who typically deliver services within licensed behavioral health agencies or facilities.
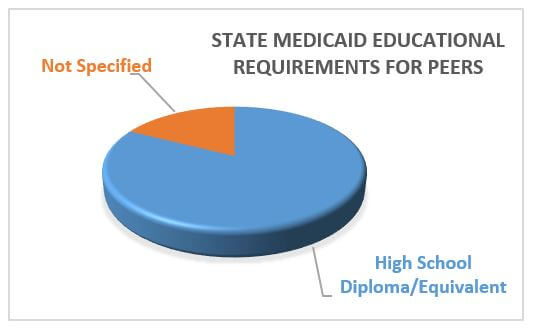
Peers are individuals with lived experience who provide Medicaid-billable SUD peer support services. NASHP identified 39 states that reimburse for 45 different types of non-licensed peers through their state Medicaid programs. No state requires more than a high school diploma (or equivalent) to become a peer, but training and supervision requirements for peers vary across states.
Key Findings
The majority of states require peers to have a high school diploma or equivalent. Thirty-two states require peers to have a high school diploma or equivalent, while six states do not specify a minimum educational requirement.
Lived experience is a universal prerequisite to working as a peer. Other peer eligibility requirements (e.g., minimum age and minimum time in recovery) vary. Some states also certify parents or other family members to provide peer services to other parents or families. Kentucky, for example, has distinct certification processes for parent, family, and youth peer support specialists serving SUD populations.
Most states require peers to participate in training or education, document their continuing education, and pass a certification exam.
State Medicaid Certification Requirements for Peers
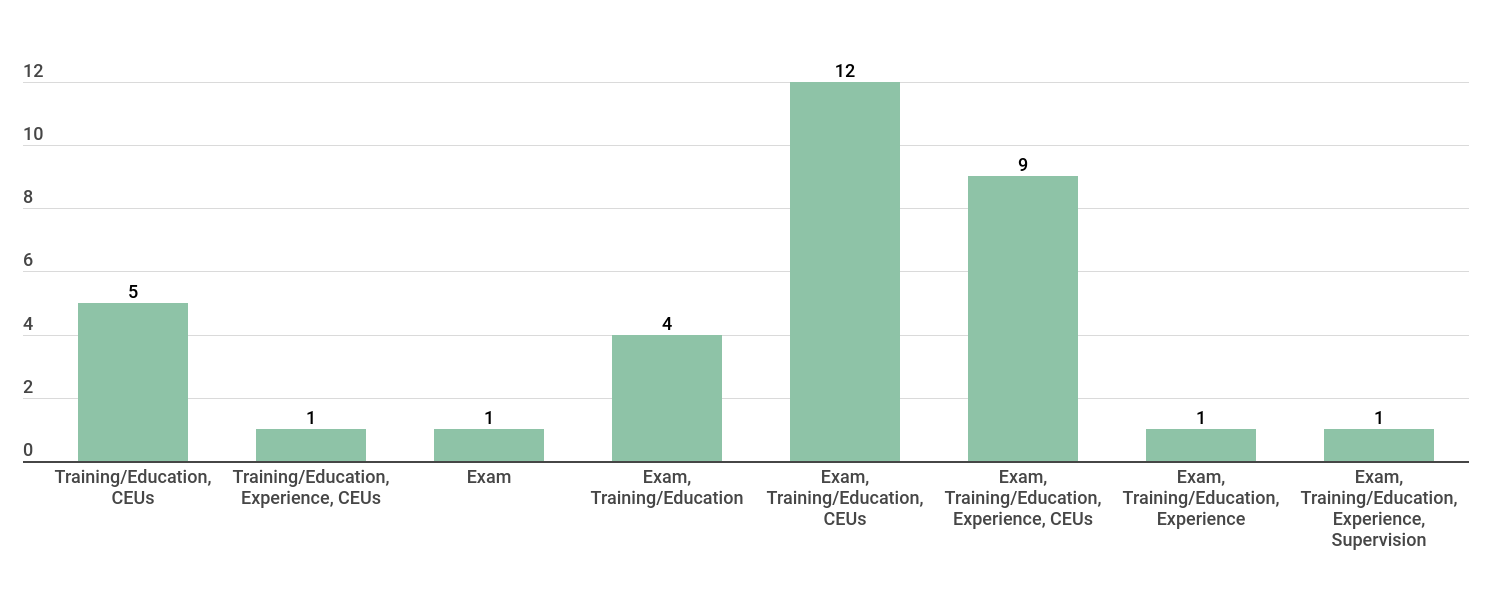
Delaware, for example, requires peers to complete a nine-day training program in addition to passing a national exam, while Ohio requires peers to complete 56 hours of training – 16 hours online, 40 hours in-person – in addition to passing a state exam.
- Twenty-seven states require peers to participate in training or education in addition to passing an exam. The exam may be a state-specific test, either the National Association of Alcoholism and Drug Abuse Counselors (NAADC) exam or the International Certification & Reciprocity Consortium (IC&RC) exam. Within these states, there are variations in the number and type of training/education and work-related experience required, and in the need for supervised practicum and continuing education;
- Five states require peers to participate in training or education, and to complete continuing education requirements;
- Four states require peers to participate in training or education; and
- One state requires passing an exam as its single requirement for peers.
The majority of states require peers to be supervised by certified or licensed SUD providers who hold at least a master’s degree. NASHP examined how states take different approaches to imposing minimum educational requirements on those who supervise non-licensed peers:
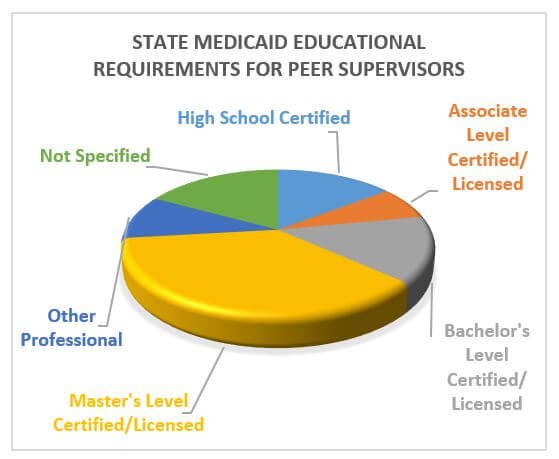 Fifteen states require supervisors to have a master’s degree and/or certification or license;
Fifteen states require supervisors to have a master’s degree and/or certification or license;
- Seven states do not have specified requirements for supervisors;
- Six states require supervisors to have a bachelor’s degree and be certified or licensed;
- Six states require supervisors to have completed high school and be certified;
- Four states require supervisors to have completed other requirements; and
- Three states require supervisors to have an associate’s degree and be certified or licensed.
Many states identify multiple eligible providers who can supervise staff, rather than requiring one specific provider type. For example, Nebraska permits its peers to be supervised by psychiatrists, licensed psychologists, provisionally licensed psychologists, advanced practice registered nurses, or nurse practitioners, in addition to numerous licensed mental health providers.
While 36 states reimburse for peer services, states often pay for additional services delivered by peers.
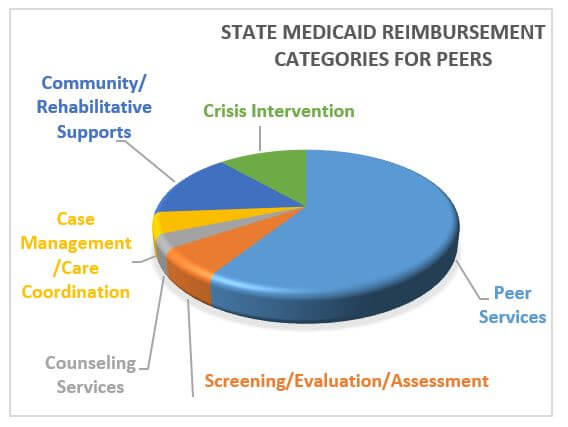
- Nine states reimburse for community/rehabilitative supports;
- Seven states reimburse for crisis intervention;
- Four states reimburse for screening, evaluation, and assessment;
- Three states reimburse for case management/care coordination; and
- Two states reimburse for counseling services.
State Medicaid programs reimburse for a variety of peer services. Peer services may include activities such as recovery support specialist services, individual peer support services, and group peer support services. For more information about the types of services included in each of these service categories, please refer to the Medicaid Reimbursement Categories Key.
Reference Data – Peers: Education, Examination, and Minimum Supervision Requirements
This chart describes the education, training, supervision, and other state requirements for non-licensed peers to deliver and be paid for Medicaid-reimbursable substance use disorder services. Reimbursements are made to licensed specialty behavioral health organizations and facilities – not to the individual provider. This data was collected from state Medicaid regulations, provider manuals, and policy guidance, state professional board websites, and other resources.
State Medicaid Requirements for Counselors
The National Academy for State Health Policy (NASHP) analyzed reports and regulations from all 50 states to identify how their state Medicaid programs reimbursed for non-licensed, non-master’s-level substance use disorder (SUD) staff – including counselors, peers, and other qualified staff – who typically deliver services within licensed behavioral health agencies or facilities.
Counselors provide Medicaid-billable SUD counseling or therapy services without a master’s degree or a state license. Based on these definitions, NASHP identified 31 states that reimburse for services delivered by 52 different types of counselors through their state Medicaid programs. Requirements related to the education, training, and supervision for these counselors vary significantly across states.
Key Findings
State Medicaid educational requirements for counselors range from no specified minimum education to a bachelor’s degree.
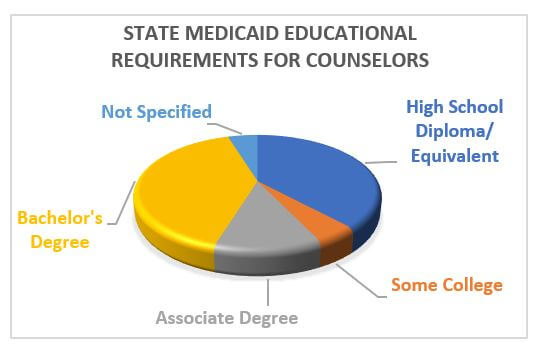 Seventeen states require counselors to have a bachelor’s degree;
Seventeen states require counselors to have a bachelor’s degree; - Sixteen require counselors to have a high school diploma or equivalent;
- Five states require counselors to have an associate’s degree;
- Two states require counselors to have some college; and
- Two states do not specify minimum educational requirements for counselors.
Some states, such as Georgia and Oregon, rank these counselors by education level (e.g., those with a high school diploma are a Counselor I and those with a college degree are a Counselor II). States vary as to whether counselors with an associate’s degree had a different designation, and whether those counselors were grouped with high school- or bachelor’s-level staff.
The majority of states require counselors to complete some training or education, acquire and document work experience and supervised practice hours, and take an exam. However, there is still significant diversity in state approaches to overseeing this SUD workforce.
State Medicaid Certification Requirements for Counselors
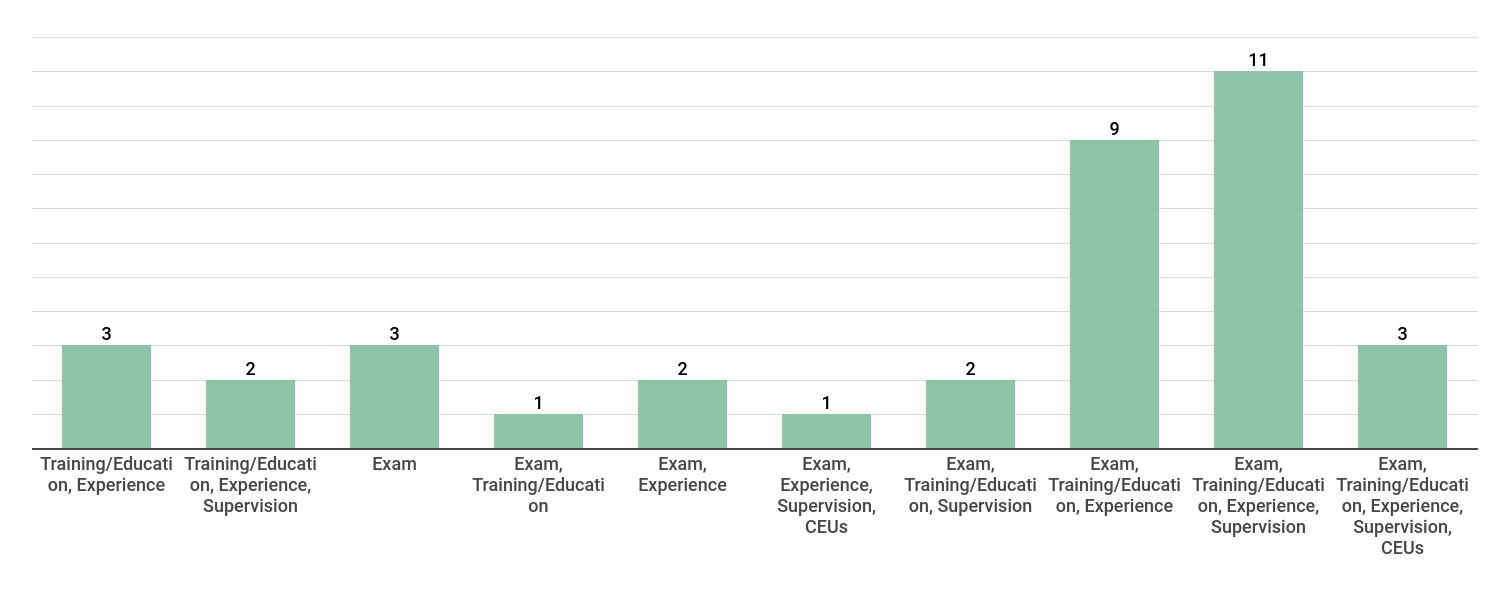
For example, Florida requires its counselors to be certified and pass its state-based exam, while Vermont requires counselors to complete at least 40 hours of substance use disorder education. New York, alternatively, requires counselors to complete both a national exam and additional training to provide administrative and clinical supervision. State Medicaid programs may also permit reimbursement for more than one level or type of counselor, each with its own requirements.
- Twenty-nine states require counselors to pass an exam in addition to completing some combination of training/education, work or volunteer experience, supervised practice, and participation in continuing education;
- Eighteen states require counselors to pass an exam, complete some training or education, and have some level of experience, but may not require additional elements such as a supervised practicum or continuing education;
- Six states do not require counselors to take an exam, but do require some combination of training/education, experience, and supervision; and
- Three states require passing an exam as its single requirement for counselors, which may be a state-specific test, the National Association of Alcoholism and Drug Abuse Counselors exam, or the International Certification & Reciprocity Consortium exam.
The majority of state Medicaid programs require non-licensed counselors to be supervised by certified or licensed SUD providers holding at least a master’s degree. NASHP examined states’ approaches with respect to the minimum educational requirements for those who supervise non-licensed counselors.
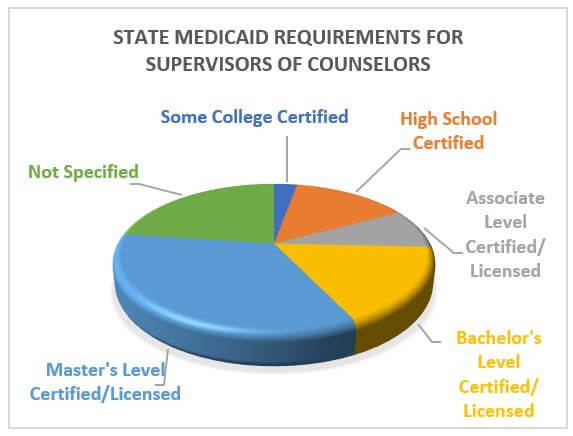 Fourteen states require supervisors to have a master’s degree and/or certification or license;
Fourteen states require supervisors to have a master’s degree and/or certification or license; - Eight states do not have specified requirements for supervisors;
- Six states require supervisors to have a bachelor’s degree and be certified or licensed;
- Five states require supervisors to have a high school diploma and be certified;
- Three states require supervisors to have an associate’s degree and be certified or licensed; and
- One state requires supervisors to have completed some college and be certified.
States reimburse for a wide variety of services delivered by counselors within licensed behavioral health settings. NASHP found that states use this non-licensed workforce to deliver a number of services across their state Medicaid SUD service array.
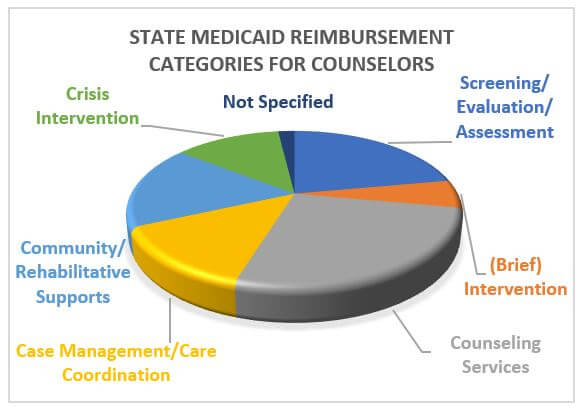 Twenty-eight states reimburse for counseling services;
Twenty-eight states reimburse for counseling services;- Twenty-three states reimburse for screening, assessment, and evaluation;
- Eighteen states reimburse for community/rehabilitative support services;
- Fourteen states reimburse for case management/care coordination;
- Thirteen states reimburse for crisis intervention; and
- Six states reimburse for brief intervention.
Within the counseling services category, most states reimburse for individual and group behavioral health therapy and counseling services. Other reimbursed services within this category include individual, family, and counseling/psychotherapy; psychoanalysis; psychotherapy for crisis; and counseling. For more information about the types of services included in each of these categories, explore the Medicaid Reimbursement Categories Key.
Reference Data – Counselor: Education, Examination, and Minimum Supervision Requirements
This chart describes the education, training, supervision, and other state requirements for non-licensed counselors to deliver and be paid for Medicaid-reimbursable substance use disorder services. Reimbursements are made to licensed specialty behavioral health organizations and facilities – not to the individual provider. The data comes from state Medicaid regulations, provider manuals, and policy guidance, state professional board websites, and other resources.
State Medicaid Requirements for Other Qualified Providers
The National Academy for State Health Policy (NASHP) analyzed reports and regulations from all 50 states to identify how their state Medicaid programs reimbursed for non-licensed, non-master’s-level substance use disorder (SUD) staff – including counselors, peers, and other qualified staff – who typically deliver services within licensed behavioral health agencies or facilities.
Other qualified staff are non-licensed professionals who provide Medicaid-billable SUD services who do not meet the definition of a peer or counselor. NASHP identified 24 states that reimburse for 43 different types of other qualified staff through their state Medicaid programs. Requirements related to the education, training, and supervision of the other qualified staff workforce sector vary significantly across states.
Key Findings
Of the state Medicaid programs that reimburse for this workforce, approximately one-third require other qualified staff to have a high school diploma or equivalent. The minimum educational requirements for other qualified staff vary across states. 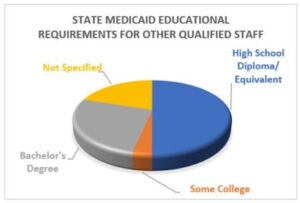
- Fifteen states require other qualified staff to have a high school diploma or equivalent;
- Eight states require other qualified staff to have a bachelor’s degree;
- Six states do not specify minimum educational requirements for other qualified staff; and
- One state requires other qualified staff to have completed some college
Of states that require a high school diploma as the minimum educational level for other qualified staff, most require some additional training and experience. Delaware, for example, requires its non-licensed credentialed behavioral health technicians to have a high school diploma and training in topics such as basic first aid, principles of recovery-oriented services, and American Society of Addiction Medicine (ASAM) criteria. States that require a bachelor’s or associate’s degree often require coursework in pertinent fields or relevant training and experience.
While the majority of states do not require this workforce to pass an exam, state approaches to certifying other qualified staff vary greatly across the country.
State Medicaid Certification Requirements for Other Qualified Staff
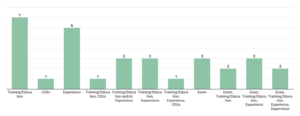
- Seven states require other qualified staff to participate in training or education;
- Six states require other qualified staff to have work-related experience;
- Three states require passing an exam as the single requirement for other qualified staff. The exam may be a state-specific test, the National Association of Alcoholism and Drug Abuse Counselors (NAADC) exam, or the International Certification & Reciprocity Consortium exam;
- Eight states require other qualified staff to meet some combination of training/education, experience, supervision, and continuing education requirements; and
- Seven states require other qualified staff to complete a combination of passing an exam and training/education, experience, and supervision requirements.
In some cases, other qualified staff may substitute education for certification or other requirements. For example, Virginia allows some other qualified staff categories to substitute a bachelor’s degree for the certification requirement. Similarly, Minnesota permits its treatment coordinators to substitute a bachelor’s degree for state certification.
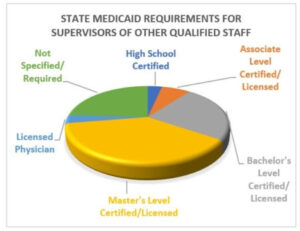
The majority of states require other qualified staff to be supervised by certified or licensed SUD providers holding at least a master’s degree. NASHP examined how states take different approaches to ongoing supervision.
- Eleven states require supervisors to have a master’s degree and/or certification or licensure;
- Seven states require supervisors to have a bachelor’s degree and be certified or licensed;
- Seven states do not specify requirements for supervisors;
- Two states require supervisors to have an associate’s degree and be certified or licensed;
- One state requires supervisors to have completed high school and be certified; and
- One state requires supervisors to be licensed physicians.
Many states identify multiple eligible providers – or categories of providers – who can supervise staff, rather than requiring one specific provider type. Nebraska takes a common approach, permitting its other qualified staff to be supervised by a licensed professional, including licensed physicians, licensed psychologists, licensed clinical social workers, licensed mental health counselors, licensed marriage and family therapists, licensed clinical addiction counselors, and other qualified behavioral health professionals.
States reimburse other qualified staff for a wide variety of services. Among the 25 states that reimburse for services delivered by other qualified staff, states pay for the following kinds of services –note that states may pay for multiple services.
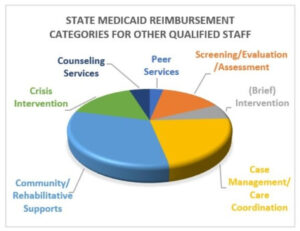
- Twenty states reimburse for community/rehabilitative support;
- Fourteen states reimburse for case management and care coordination;
- Ten states reimburse for crisis intervention;
- Nine states reimburse for screening, assessment, and evaluation;
- Four states reimburse for brief intervention;
- Three states reimburse for counseling services; and
- Two states reimburse for peer services.
Other qualified staff perform a range of care coordination and case management functions. Services reimbursed by state Medicaid agencies include service plan development, SUD case management, ongoing case management, targeted case management, and targeted plan development. For more information regarding these service categories, view the Medicaid Reimbursement Categories Key.
Reference Data – Other Qualified Staff: Education, Examination, and Minimum Supervision Requirements
This chart describes the education, training, supervision, and other state requirements for non-licensed staff to deliver and be paid for Medicaid-reimbursable substance use disorder services. Reimbursements are made to licensed specialty behavioral health organizations and facilities – not to the individual provider. The data comes from state Medicaid regulations, provider manuals, and policy guidance, state professional board websites, and similar resources.
Medicaid Reimbursement Categories Key
Peer Services
H0038 – Peer Support Services
H2015 – Recovery Support Specialist Service
H2016 – Comprehensive Community Support Services (Peer), per diem
S9445 – Group Peer Support Services
T1012 – Individual Peer Support Services
Screening/Evaluation/Assessment
90791 – Psychiatric Diagnostic Evaluation/Intake Interview
96127 – Brief Assessment
99408 – SBIRT/Screening (15-30 mins)
99409 – SBIRT/Screening (30+ mins)
H0001 – Alcohol and/or Drug Assessment
H0002 – Behavioral Health Screening to Determine Admission Eligibility; Extended Assessment (75+ mins); Screening and Referral
H0031 – Behavioral/Mental Health Assessment by Non-Physician
H0049 – Screening
H2000 – Comprehensive Assessment
T1011 – Evaluation/Determination of Placement
T1023 – Program Intake Assessment; Brief Assessment
Brief Intervention
99408 – SBIRT
H0004 – Brief Treatment
H0022 – Alcohol and/or Drug Intervention Services; Early Intervention
H0049 – Screening and Intervention (less than 15 mins)
H0050 – Brief Intervention
Counseling Services
90832 – Individual Counseling/Psychotherapy, 30 mins (16-37 mins)
90834 – Individual Counseling/Psychotherapy, 45 mins (38-52 mins)
90837 – Individual Counseling/Psychotherapy, 60 mins (53+ mins)
90839 – Psychotherapy for Crisis, first 60 mins
90840 – Psychotherapy for Crisis, additional 30 mins
90485 – Psychoanalysis
90846 – Family Counseling/Psychotherapy (without client)
90847 – Family Counseling/Psychotherapy (with client)
90849 – Multiple Family Counseling/Psychotherapy
90853 – Group (non-family) Counseling/Psychotherapy
90877 – Collateral Therapy/Family Consultation
96153 – Group Therapy
96154 – Family Therapy (with client)
96155 – Family Therapy (without client)
99354 – Prolonged Individual Counseling/Psychotherapy Service (additional 30-60 mins)
99355 – Additional Prolonged Individual Counseling/Psychotherapy Service (per 15-30 mins)
H0004 – Individual Behavioral Health Therapy and Counseling
H0005 – Group/Family Counseling
H2019 – Individual/Group Therapy
G0396 – Substance Use Disorder Counseling (25-45 mins)
G0397 – Substance Use Disorder Counseling (45+ mins)
T1006 – Family/Couple Counseling
Community/Rehabilitative Supports
H0025 – Behavioral Health Prevention Education
H0034 – Medication Monitoring/Training/Support
H0036 – Basic Living Skills Training
H0043 – Supported Housing
H2014 – Individual/Family Skills Training and Development; Behavioral Modification
H2015 – Comprehensive Community Support Services; Addictive Diseases Support Services
H2017 – Individual/Group Psychosocial Rehabilitative Services; Living Skills Training
H2019 – Individual/Family Therapeutic Behavioral Services
H2022 – Intensive In-Home Services
H2025 – Supported Employment
H2026 – Supported Employment (per diem)
H2027 – Psychoeducational Services; Didactic Counseling
S5110 – Family Support (Home Care Training)
S5111 – Family Support and Training
S9482 – Family Support
T1012 – (Non-Peer) Recovery Support; Family Education
T1019 – Personal Care Services
T1020 – Personal Care Services (per diem)
Case Management/Care Coordination
H0006 – Substance Use Disorder Case Management
H0032 – Service Plan Development
H2036 – Recovery Navigation Support
G9012 – Substance Use Care Coordination; Ongoing Case Management
T1007 – Treatment Plan Development
T1016 – Case Management; Treatment Coordination
T1017 – Case Management; Targeted Case Management
T2023 – Targeted Case Management
Crisis Intervention
90791 – Crisis Evaluation
90839 – 24 Hour Access to Crisis Response, first 60 mins
90840 – 24 Hour Access to Crisis Response, additional 30 mins
99510 – Mobile Crisis Response
H2011 – Crisis Intervention/Management/Follow-up; Mobile Crisis Management
H2018 – Crisis Residential Services
S9484 – Crisis Stabilization/Intervention; Crisis Service Center; Mobile Crisis Service
S9485 – Crisis Stabilization (per diem)
Bundles
H0010 – Subacute Detoxification (Residential Setting) (ASAM 3.2-WM); High Intensity Residential Treatment; Clinically Managed Residential Treatment (ASAM 3.3; 3.5)
H0011 – Acute Detoxification (Residential Setting) (ASAM 3.7-WM); Medically-Managed Residential Treatment (ASAM 4)
H0012 – Subacute Detoxification (Outpatient Setting) (ASAM 2-WM); Non-Medical Community Residential Treatment (ASAM 3.5)
H0013 – Outpatient Detoxification (Residential Setting) (ASAM 2-WM); Medically Monitored Community Residential Treatment (ASAM 3.7)
H0014 – Outpatient Detoxification (Ambulatory Setting) (ASAM 2-WM)
H0015 – Intensive Outpatient Program (ASAM 2)
H0018 – Short-Term Residential Services; Medically Monitored Intensive Residential Treatment (ASAM 3.7); Residential Treatment Program with 17+ beds
H0019 – Long-Term Residential Services; Clinically Managed High-Intensity Residential Treatment (ASAM 3.5)
H0035 – Partial Hospitalization (ASAM 2.5)
H0043 – Residential Alcohol and Drug Services (ASAM 3)
H2001 – Outpatient Rehabilitation (2-4 hours)
H2012 – Day Treatment (≤5 hours) (ASAM 2.1)
H2015 – Day Treatment (after 5 hours) (ASAM 2.5)
H0020 – Opioid Treatment Program
H2034 – Low-Intensity Residential Treatment/Halfway House (ASAM 3.1)
H2035 – Outpatient Alcohol and/or Drug Treatment Services
H2036 – High-Intensity Residential Treatment (ASAM 3.3/3.5/3.7); Outpatient Alcohol and/or Drug Treatment Service, per diem/>4 hours; Medically Supervised Detoxification Crisis Stabilization (ASAM 3.7-WM); Residential Treatment Program with <16 beds; Residential Treatment Program (ASAM 3.1/3.3/3.5/3.7)
S0201 – Partial Hospitalization Services in Acute Care or Psychiatric Hospital; Partial Hospitalization Services (ASAM 2.5)
S2080 – Health Home initial Recovery Action Plan
S2081 – Health Home Ongoing Care Management
S9480 – Intensive Outpatient Program
Notes
[1] “Medicaid Works for People with Substance Use Disorders,” Center on Budget and Policy Priorities, January 19, 2018, https://www.cbpp.org/sites/default/files/atoms/files/1-19-18health-factsheet-suds.pdf.
[2] Ellen Bouchery, and Judith Dey, “ASPE Issue Brief: Substance Use Disorder Workforce,” HHS Office of the Assistant Secretary for Planning and Evaluation, June, 2018, https://aspe.hhs.gov/system/files/pdf/259346/ExamSUDib.pdf.
[3] Angela J. Bech, Cory Page, Jessica Buche, Danielle Rittman, and Maria Gaiser, “Scopes of Practice and Reimbursement Patterns of Addiction Counselors, Community Health Workers, and Peer Recovery Specialists in the Behavioral Health Workforce,” Behavioral Health Workforce Research Center, University of Michigan School of Public Health, http://www.behavioralhealthworkforce.org/wp-content/uploads/2019/06/Y3-FA3-P1-SOP-Full-Report-Updated-6.5.19.pdf.
[4] Elizabeth Hinton, MaryBeth Musumeci, Robin Rudowitz, Larisa Antonisse, and Cornelia Hall, “Section 1115 Medicaid Demonstration Waivers: The Current Landscape of Approved and Pending Waivers,” Kaiser Family Foundation, February 12, 2019, https://www.kff.org/medicaid/issue-brief/section-1115-medicaid-demonstration-waivers-the-current-landscape-of-approved-and-pending-waivers/.
[5] Angela J. Bech, Cory Page, Jessica Buche, Danielle Rittman, and Maria Gaiser, “Scopes of Practice and Reimbursement Patterns of Addiction Counselors, Community Health Workers, and Peer Recovery Specialists in the Behavioral Health Workforce,” Behavioral Health Workforce Research Center, University of Michigan School of Public Health, http://www.behavioralhealthworkforce.org/wp-content/uploads/2019/06/Y3-FA3-P1-SOP-Full-Report-Updated-6.5.19.pdf.
[6] Elizabeth Hinton, MaryBeth Musumeci, Robin Rudowitz, Larisa Antonisse, and Cornelia Hall, “Section 1115 Medicaid Demonstration Waivers: The Current Landscape of Approved and Pending Waivers,” Kaiser Family Foundation, February 12, 2019, https://www.kff.org/medicaid/issue-brief/section-1115-medicaid-demonstration-waivers-the-current-landscape-of-approved-and-pending-waivers/.
Acknowledgments: The National Academy for State Health Policy (NASHP) would like to thank state officials who generously shared their time and insights in reviewing this material. The authors also thank Trish Riley and Jodi Manz of NASHP, as well as Lynnette Araki and her colleagues at the Health Resources and Services Administration for their guidance and helpful feedback.
This project was supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under grant number UD3OA22891, National Organizations of State and Local Officials. The information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the US government.


