 As state policy leaders work to improve quality and reduce cost in the management of public health systems, ensuring access to the full continuum of support for people with serious illness may be an underutilized approach to achieving value in state health care spending, particularly within Medicaid managed care.
As state policy leaders work to improve quality and reduce cost in the management of public health systems, ensuring access to the full continuum of support for people with serious illness may be an underutilized approach to achieving value in state health care spending, particularly within Medicaid managed care.
Research recently published in the Journal of the American Medical Association found that even oncologists taking care of patients with stage IV cancer largely missed opportunities to discuss advance care planning, palliative care, and end-of-life decisions with their seriously ill patients. This finding confirms major takeaways from the 2015 Institute of Medicine landmark work Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life. The report underscores that care received by people with serious illness is fragmented and uncoordinated, often fails to address pain and other symptoms, typically involves multiple transitions across care settings, and may not reflect the wishes of the individual and their family.
People with serious and life-threatening health conditions experience care needs that drive costs, including hospital admissions, emergency department utilization, and nursing home care. State Medicaid programs invest significant resources on care for beneficiaries with serious illness: roughly $11 billion to treat cancer, $51 billion on Alzheimer’s disease and other dementias, and $12.2 billion on chronic obstructive pulmonary disease (COPD) per year. Well-coordinated care that anticipates and manages the symptoms and stressors of serious illness can help people with these and other complex conditions reduce pain and suffering, avoid receiving treatment that does not align with their wishes, and prevent overutilization of care.
In addition to providing curative treatment, the continuum of care for complex and serious illness incorporates palliative care, a team-based, coordinated set of services and supports that includes:
- Advance care planning
- Discussion of individual goals of care and assistance with decision-making
- Assessment and management of pain and other symptoms
- Comprehensive care coordination
- Behavioral and/or spiritual supports for the individual and family
As Medicaid managed care becomes the predominant delivery system for Medicaid populations, states can look to contracts with managed care organizations (MCOs) and plan expertise as a way to build and enhance the continuum of care for people with serious illness. States, through MCOs contracts providing acute care, long-term care, as well as Dual Eligible Special Needs Plans (D-SNPs), and other managed care vehicles, have a range of strategies they can use to enhance care for populations with serious illness.
State Strategies
In recent years, policymakers have paid particular attention to Medicaid managed care enrollees with chronic illness — individuals who typically have multiple comorbid conditions, functional disability, and require significant Medicaid resources over a long period of time. There is substantial overlap between this population and those enrollees with serious illness; individuals who could benefit from palliative care may include patients with life-threatening illnesses, as well as individuals with chronic conditions that worsen over time. Building on existing state strategies can ensure appropriate supports across this continuum of care.
Delivery system transformation: Leading states such as Minnesota have long used Medicaid MCO contracts to address the needs of complex populations and those with serious illness. Since 2014 (first under its “Dual Demo” demonstration and then later via D-SNP contracts), the state has enabled Medicaid MCOs to participate in value-based purchasing through its Integrated Care System Partnerships (ICSP) model. ICSP is a flexible, integrated approach with a focus on improving care coordination and creating linkages across primary, acute, and long-term care for people with complex needs. Through ICSPs, plans may propose and develop diverse care models that address the needs of particular populations. Minnesota provides a menu of quality measures that plans may select to qualify for value-based payments; plans may also develop and propose their own. In addition to a range of metrics related to promoting prevention and reducing utilization related to ambulatory care-sensitive conditions, ICSP measures have included advanced care planning, evidence of physician order for life-sustaining treatment (POLST), effective care transitions, and assessment and management of chronic pain. The model is based on Minnesota’s successful Integrated Health Partnerships model, which includes a shared savings/losses option that has resulted in over $400 million in savings to the state compared to expected costs between its inception in 2013 and 2019.
Rhode Island is another state that has invested in coordinated care for complex populations enrolled in Medicaid. Rhode Island’s Financial Alignment Initiative demonstration program, the Integrated Care Initiative, offers intensive coordination and supports for dual eligible individuals with significant needs. The state and U.S. Department of Health and Human Services jointly contract with the Neighborhood Health Plan of Rhode Island; payment to the plan is based in part on plan performance on a slate of federal and state measures, including Care for Older Adults, which reports the number of older adults who have received medication review, functional status assessment, pain assessment, and advance care planning.
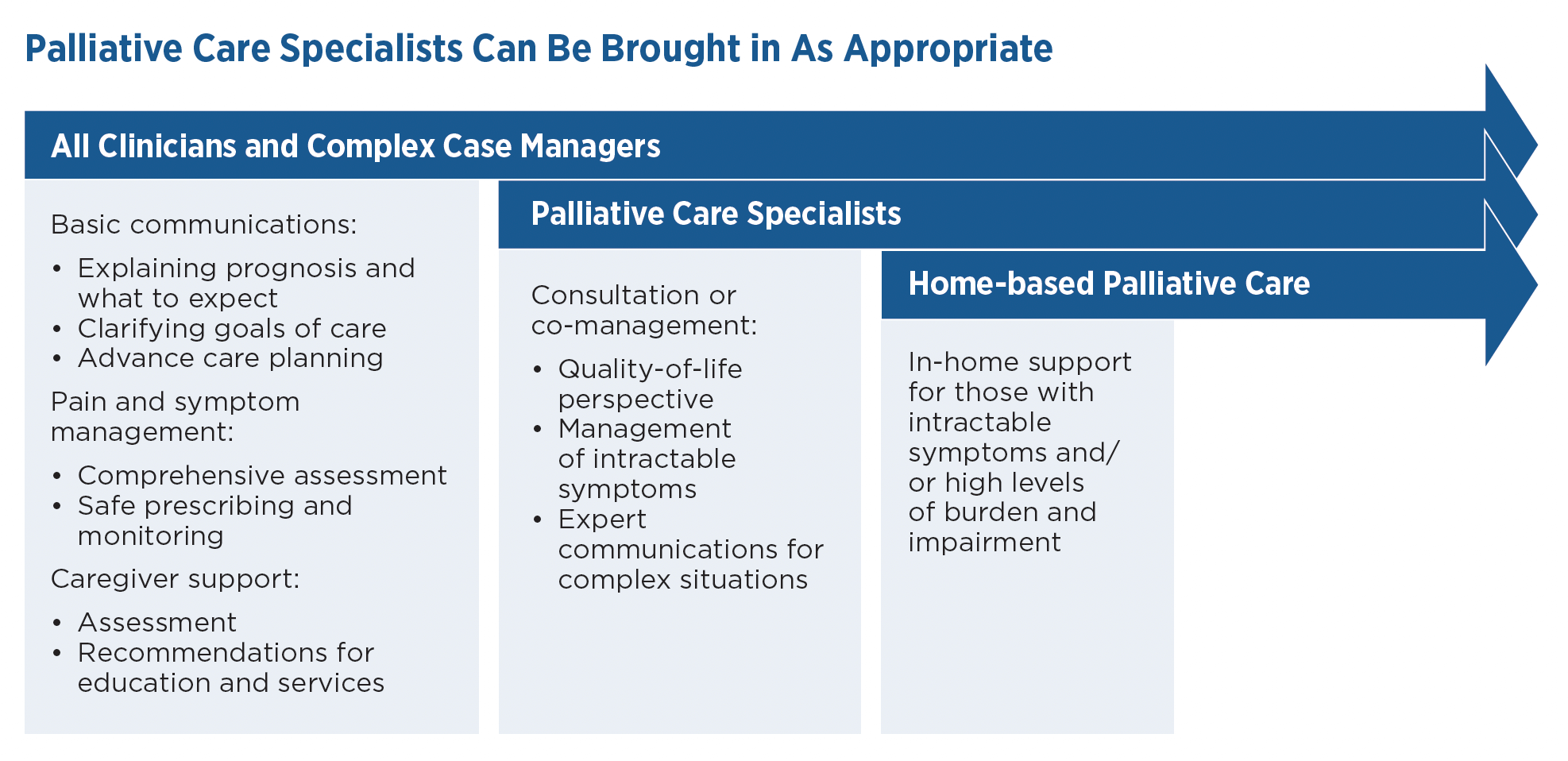
Palliative care benefits: States may enhance the continuum of care for people with serious illness by ensuring that palliative care benefits are included in contracts with Medicaid MCOs. Policymakers may want to build palliative services into particular settings (outpatient, in-home) or structure medical necessity criteria to focus on certain high-need patient populations. Figure I describes the range of palliative care capacity across general practitioners, home-based and specialty palliative care, and hospice:
California was an early leader in supporting palliative care through its Medicaid MMO contracts; SB 1004 required the Department of Health Care Services (DHCS) to provide standards and technical assistance for MCOs in Medi-Cal, California’s Medicaid Program, on the provision of palliative care. DHCS issued guidance to MCOs on the types of services that must be included as part of the palliative care benefit, the minimum diagnoses to be covered (congestive heart failure, chronic obstructive pulmonary disease, advanced cancer, liver disease), and the types of providers and settings that could provide palliative care. SB 1004 requires DHCS to ensure that delivery of these services is as cost-neutral as practicable. In developing the benefit, the state leveraged existing billing codes, ensuring that services could be billed under existing state plan benefits. This avoided the need to submit a state plan amendment for federal approval for a specific palliative care benefit.
States are typically required to cover Medicaid state plan services under the MCO contract and build those costs into actuarially sound capitation rates. Arizona’s End of Life and Advanced Care Planning benefit is referenced in its MCO contracts and further described in state regulations. The goal of the benefit is “relief of stress, pain, or life limiting effects of illness to improve quality of life for a member at any age who is currently or is expected to experience declining health or is diagnosed with a chronic, complex, or terminal illness.” Services may include treating the underlying illness as well as relieving pain and stress and providing referral to pastoral, counseling, and legal services. Adults may receive benefits along with curative care until they choose to receive hospice. Children may access services along with both curative and hospice care.
Identifying populations with serious illness: Definitions for serious illness vary. From a practical perspective, “serious illness,” “chronic illness,” “complex conditions,” and similar terms are used within state policies to describe populations that — to improve care and reduce cost — may benefit from additional supports. States can build on existing MCO contract definitions to ensure that individuals with serious illness are identified and able to access care that can both relieve symptoms and avoid unnecessary or unwanted interventions. As with other complex populations, diagnoses alone may not precisely identify enrollees who might benefit from palliative care services and supports.
- Focus on function and utilization, in addition to diagnoses. States such as Delaware have built inclusive definitions into their MCO contracts that help to identify enrollees with serious illness who may require additional supports. Medicaid MCOs are required to identify populations with a “history of poor outcomes, utilization patterns that suggest inadequate linkage to primary and preventive care, or other indicators of high risk or potential for poor health outcomes.” For members identified as having serious health care needs, plans must provide a comprehensive assessment within 30 days, and referral to a clinical care coordination program.
- Use screening tools. States can require plans to use screening tools to identify members with significant needs. Virginia’s Member Health Screening Survey includes questions to identify medically complex members, including diagnoses and how conditions affect activities of daily living. Members identified as having significant needs not already enrolled in Commonwealth Coordinated Care Plus program are enrolled in the program.
- Leverage data. Texas supports the Texas Healthcare Learning Collaborative Portal, an interactive repository of data from Medicaid MCOs and other sources. The portal includes a “super-utilizer dashboard” with data sets that can be sorted to identify patterns of emergency department and inpatient utilization.
- Ensure timely identification. To fully benefit from palliative care, individuals are ideally identified before crises occur. West Virginia’s contract with their MCOs requires the plans to have procedures for identifying individuals with “complex or serious medical conditions.” MCOs must complete identification and assessment within 90 days of the effective date of enrollment. MCOs must also share assessment with other plans working with the individual to facilitate care coordination, and develop a treatment plan incorporating the individual’s identified needs.
Care planning/care management: Care planning/care management activities represent key contact points with Medicaid enrollees, offering opportunities for plans (and/or contracted providers) to identify individuals with serious illness, discuss treatment goals, and address palliative care needs:
- Include pain and symptoms in assessment and care planning. While the majority of state MCO contracts do not call out pain or symptom management in contract protocols for care coordination/care management, some states are making sure that these issues are routinely addressed as part of the MCO’s role. Indiana’s acute MCO contract requires plans to have protocols “to assess, plan, implement, re-assess and evaluate members,” including pain and advance care planning. Arizona’s disease management definition in its Medicaid MCO contract notes the need to include symptom management and engage with enrollees on health-related goals. In Rhode Island, MCO plans of care must include “interventions to address special needs (e.g., pain management, cognitive impairment, physical/vocational/speech therapy).”
- Enhance federal advance care planning requirements. Federal Medicaid managed care regulation requires that MCOs provide enrollees with information about advance directives. Washington, through the state’s Apple Health Integrated Managed Care contract, provides comprehensive guidance to its MCOs on supporting individuals in advance care planning and completion of Physician Orders for Life-Sustaining Treatment (POLST), a medical order form that expresses members’ treatment wishes to health care providers. Plans must develop procedures to share information on POLST forms, include family members in planning discussions if the member is incapacitated, document in the medical record whether or not an enrollee has an advance directive or POLST in place, and provide education to staff. Other states, such as New Mexico’s sample contract for Centennial Care 2.0, which includes both acute care and long-term services and supports (LTSS), require training on advance directives/end-of-life care for new care coordinators.
- Incorporate goals of care into person-centered planning. Person-centered planning is a core principle in state home and community-based services systems and is embedded in state managed long-term services and supports contracts (see “Principles for Person-Directed Services and Supports during Serious Illness,” a resource for policymakers, plans, and care managers, below). States can build on this critical function by ensuring that individuals are actively supported to plan for serious illness and anticipate end-of-life needs.
Principles for Person-Directed Services and Supports during Serious Illness
| GOALS | PRINCIPLES |
|---|---|
| 1. Promote choice and control for people with serious illness, while taking into account their unique life circumstances; 2. Help people plan for serious illness; 3. Help families, family caregivers, and service providers honor the choices of people with serious illness; and 4. Assist people with serious illness in choosing and controlling services according to personal values, priorities, and goals. |
• Live with serious illness according to personal values and goals, including the place where they live • Enable choice of services, i.e., to choose or decline services • Avoid discrimination • Enable choice of representative, including family or friends • Carry out person-directed planning and decision-making for priorities, goals, and needs • Access to care coordination • Choice of services and supports • Deliver palliative care • Provide hospice care • Provide independent advocacy services, especially for legal matters • Educate and support providers, e.g., communication and pain/symptom management • Support family caregivers through a consistent care coordination team, access to a 24 hour/7 day a week helpline, emergency back-up, respite care, grief counseling, and information/referral to community services • Address the concerns of older adults; people with disabilities, including those with developmental disabilities; and their family caregivers |
Source: U.S. Administration for Community Living, August 30, 2017. Accessed at https://acl.gov/sites/default/files/Aging%20and%20Disability%20in%20America/Serious%20Illness%20Principles%208-30-17%20508%20compliant.pdf.
Quality and performance measures. As part of contract and systems oversight, states engage in a range of quality assessment and improvement strategies. Federal state and regulations require that states track the quality of care received by enrollees and particularly the care received by enrollees with special health care needs. Using quality measures and performance improvement projects that focus on serious illness can help states understand the value and uptake of these services.
Select Measures for Serious Illness Care
| QUALITY DOMAIN | MEASURES | SOURCES |
|---|---|---|
| Patient Satisfaction | • CAHPS (Consumer Assessment of Health Providers and Systems) [multiple survey options] • Likelihood to recommend the services or program (i.e., Net Promoter Score) |
CAHPS |
| Advanced Care Planning | • Rates of patients who have an advance care plan or surrogate decision-maker documented in the medical record or documentation in the medical record that an advance care plan was discussed | NQF: 0326 |
| Healthcare Effectiveness Data and Information Set (HEDIS) Care for Older Adults | Percentage of beneficiaries age 66 and older who had four critical services in one measurement year: • Advance care planning • Medication review • Functional status assessment • Pain screening |
NCQA |
States are beginning to adopt these and related measures, largely within Medicaid managed long-term care contracts. For example, Illinois’ Financial Alignment Demonstration, which supports dual eligible beneficiaries, uses the Healthcare Effectiveness Data and Information Set (HEDIS) Care for Older Adults measure. Both Ohio and Rhode Island include the HEDIS Measure of Care for Older Adults in their managed long-term care contracts. Virginia has adopted an advance care planning measure within its CCC Plus MLTSS contract.
Key Takeaways for States
Build on existing strategies. Policymakers across states have developed successful processes and capacity to better manage the needs of people with chronic conditions through MCO contracts. Palliative care can build on and reinforce this work. Leveraging clinical models, population-based care approaches, care management, and other MCO features, states may want to consider expanding the continuum of care for people with serious illness by modifying existing contract language.
Managed LTSS (MLTSS) contracting may be a particular opportunity for states. People enrolled in MLTSS programs often have serious and life-threatening conditions such as Alzheimer’s disease, diabetes, and COPD — conditions that can often benefit from palliative care interventions. To support access to this care, states can consider requiring MLTSS plans to ensure that home and community-based service providers have core palliative care communication skills, that managing the symptoms of serious illness is addressed within care plans, and that specialty palliative care is available for referral when needed. Additional opportunities may be available to states when partnering with Dual Eligible Special Needs Plans (D-SNPs) for Medicaid MLTSS services. Recent changes in federal Medicare guidance permit Medicare Advantage plans (including D-SNPs) to provide home-based palliative care as a supplemental benefit. This change could expand the continuum of care for people with serious illness beyond the traditional Medicare hospice benefit, which is time-limited and generally underutilized.
Commercial plans are leading the way. The Center to Advance Palliative Care notes significant activity among commercial plans to support palliative care. Aetna’s Compassionate Care Program offers palliative supports, such as care management and advance care planning, for people with serious illness and their families. Anthem and Highmark have incorporated palliative care access measures within value-based payment programs. SCAN Health Plan has launched a model with complex care supports for those in assisted living and skilled nursing facilities. In 2018, Blue Shield of California expanded its home-based palliative care program to provide the service statewide. Policymakers in leading states note that market forces and increasing palliative care capacity have influenced their states’ interest in supporting a Medicaid palliative care benefit. These and other models from the commercial sector can help build network capacity and provide lessons for states.
Conclusion
While state support for palliative care services is still emerging, Medicaid managed care contracts may be a fertile area for targeted state action. Building on existing work by states and plans, palliative care can provide an additional strategy for states seeking to improve the care of complex populations, while reducing cost.
Acknowledgments
The authors thank Rani Snyder, Amy Berman and Scott Bane (The John A. Hartford Foundation); Torrie Fields (Votive Health); Allison Silvers and Stacie Sinclair (Center to Advance Palliative Care), and policy makers from the states of South Carolina, Hawaii, and Minnesota.
This brief was supported by a generous grant from The John A. Hartford Foundation and is part of NASHP’s initiative, Expanding and Sustaining the Continuum of Care: A Resource Hub for State Policymakers.


