To address the ongoing challenges of the opioid and overdose crisis, states are considering how to most effectively target various funding sources to provide treatment and recovery services for opioid use disorder (OUD) and substance use disorder (SUD). Funding from the Medicaid program and the Substance Abuse and Mental Health Services Administration (SAMHSA) comprise the majority of spending on SUD treatment but may be supplemented by opioid settlement funds, state funding, and other federal grant programs that serve populations with SUD.
Understanding where investments are already being made can help to better target the use of new funding and resources. An organized approach for assessing and tracking multiple funding streams, through different state agencies and different parts of state budgets, can help state agencies strategically align resources to support a full continuum of SUD services.
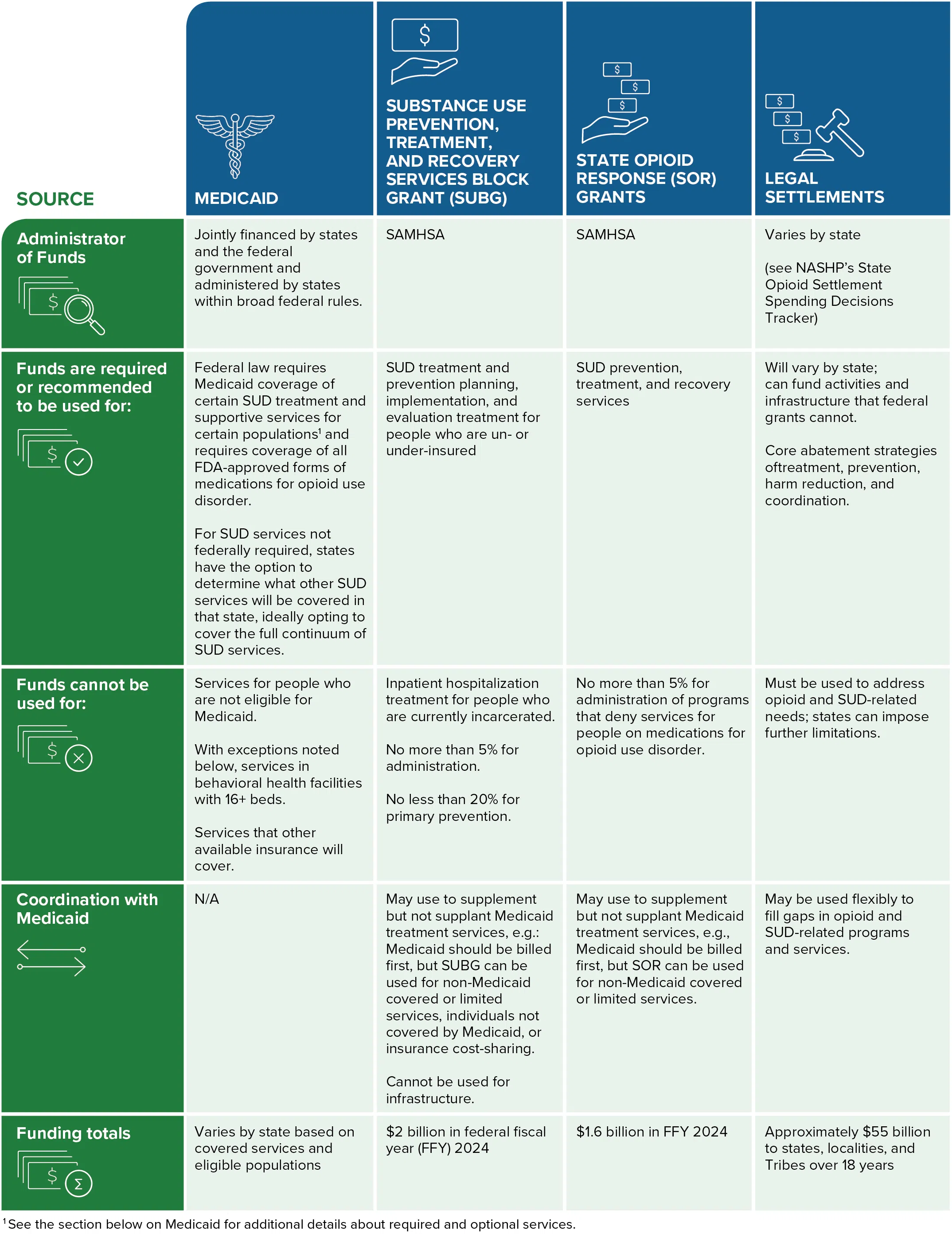
State Funding Sources for SUD Treatment
Key Funding Sources
1. Medicaid
Federal data indicate that 8.1 percent of all individuals enrolled in Medicaid received SUD treatment services in 2020 and that Medicaid is the single largest payer of behavioral health services in the U.S. Unlike other funding sources, Medicaid guarantees coverage of services to individuals who qualify.
Medicaid is jointly financed by the Centers for Medicare and Medicaid Services (CMS), and each state Medicaid agency administers its program, with significant flexibility to design the coverage and financing of services, within broad requirements set by CMS. State Medicaid programs are required to cover all drugs approved by the U.S. Food and Drug Administration (FDA) for the treatment of opioid use disorders and related counseling services and behavioral health therapies; mental health and SUD treatments services for individuals eligible through Medicaid expansion; and medically necessary SUD services through the early and periodic screening, diagnostic, and treatment benefit for children. Increasingly, states are covering optional SUD services to create a full continuum of care.
Federal Resources on Medicaid and SUD
Key Requirements and Limitations
- Services are available to people who are categorically and financially eligible for and enrolled in state Medicaid programs.
- Covered services. In addition to mandated services described above, states have the flexibility to determine coverage of a variety of SUD treatment and recovery supports, including counseling, withdrawal management, medication-assisted treatment, intensive outpatient programs, case management, peer supports, skills training and development, supported employment, and supported housing.
- Medication coverage. Per the Substance Use Disorder Prevention that Promotes Recovery and Treatment (SUPPORT) Act, state Medicaid programs must cover all three forms of medications for opioid use disorder (MOUD).
- Institutes of Mental Disease (IMD) exclusion. While states are statutorily precluded from coverage of services in IMDs under Medicaid (defined in the Social Security Act as hospitals, nursing facilities, or other institutions with over 16 beds that primarily treat mental health conditions), a time-limited state plan option established through section 1915(l) of the SUPPORT Act allows for coverage of IMD services. The SUPPORT Act also created an exception for states to allow Medicaid coverage of SUD treatment for pregnant and postpartum individuals in IMDs. States can also request an exception to the IMD exclusion through Medicaid Section 1115 demonstration waivers.
- Inmate exclusion. Individuals who are incarcerated are ineligible for Medicaid coverage, except for inpatient hospital services, meaning that jails and prisons must use other funds to address SUD treatment needs. In 2023, CMS introduced the Medicaid Reentry Section 1115 Demonstration Opportunity to support states’ efforts to provide additional supports during the reentry period. The opportunity allows state Medicaid programs to cover various health services, including SUD treatment for a period of time immediately prior to release and a supply of medications at release — as of January 2025, 19 states have approved reentry demonstration waivers.
- Health-Related Social Needs. Medicaid state plans can cover a variety of health-related social needs and recovery supports, including supported housing and employment, peer services, family peer services, respite services, and case management. As of January 2025, 15 states have approved Section 1115 demonstration waivers allowing short-term rental assistance and nutrition services coverage. Learn more about Medicaid and housing supports through NASHP’s toolkit.
2. Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG)
These non-competitive federal block grants were established in 1993. Funding to states totaled $2 billion in federal fiscal year (FFY) 2024 to support planning, implementation, and evaluation for prevention and treatment activities for all substance use disorders. Single state agencies for behavioral health are required to administer these funds in states.
Key Requirements and limitations (per SAMHSA)
- No more than 5 percent of funding may be used for administrative costs. SAMHSA also requires a 5 percent set-aside for data collection and other technical assistance activities.
- Primary prevention. States must use no less than 20 percent of SUBG funds for primary prevention efforts for individuals who do not yet meet criteria for SUD but are at risk.
- Treatment and prevention. States must use the remaining 70 percent of funds for both alcohol use disorder (AUD) and other SUD prevention, early intervention, treatment, and recovery. States can use SUBG dollars to fund treatment services for individuals who are uninsured or who are experiencing gaps in coverage or for SUD services not covered under insurance. However, these funds are restricted from paying for inpatient hospitalization and treatment in incarceration settings.
- Coordination with Medicaid. States may use SUBG funds to supplement, but not supplant, Medicaid coverage for treatment services. SUBG covers gaps in payment to providers for non-covered or limited Medicaid services that have demonstrated effectiveness. SAMHSA has also provided guidance for states indicating that SUBG funds may also be used to cover Medicaid spend-down for individuals, as well as cost-sharing requirements for individuals with private insurance for SUD treatment services.
3. State Opioid Response (SOR) Grants
SOR grants are non-competitive, two-year federal grants that totaled $1.6 billion in FFY 2024. SOR funds can be used to support opioid and other SUD-related activities in states and are administered by SAMHSA to each state on a needs-based formula methodology. In addition to administering SUBG funds, SSAs are also required to administer these funds in states.
Requirements and limitations (per SAMHSA)
- Funds must be used to supplement existing SUD-related activities and programs in states and cannot be used to supplant other federal funds. This presents an opportunity for states to fund treatment for individuals and services not eligible for Medicaid reimbursement. States must use SOR grants to implement not only treatment, but community recovery supports and prevention activities as well, including for individuals transitioning into the community from incarceration or institutional settings.
- No more than 5 percent of funds can be used for administrative and infrastructure purposes, although up to 2 percent can be used for data collection.
- States may only use funds for FDA-approved forms of MOUD. Further, states may not use funds toward programs or sub-awardees that deny services to individuals on prescribed MOUD for treatment.
- Medicaid interaction. States can use SOR funds to provide treatment services but cannot use these funds to supplant other resources. Providers are generally directed to bill Medicaid for eligible patients/services first and use these funds to supplement billable treatment services.
4. Opioid Settlements
States and localities are in the process of implementing structures and plans to distribute upwards of $55 billion from opioid-related lawsuits. Through each state’s unique settlement process, states and localities are in the process of identifying priorities and making investments in SUD prevention, treatment, and recovery infrastructure.
See NASHP’s Opioid Settlement Spending Decision Tracker for information on state spending decisions, as well as state-by-state information on each state’s settlement-related laws, agreements, processes, reports, and spending dashboards.
Requirements and limitations
The terms of the National Settlement, which at $26 billion is the largest source of opioid settlement funding flowing to states, requires that at least 70% of funding must be spent on current and future “opioid remediation efforts,” which include programs and expenditures to address the misuse of opioid products, treat opioid use and related disorders, and mitigate the effects of the opioid epidemic.
Each state has set up its own unique process for deciding how various opioid settlement award funds will be divided and spent across agencies, abatement funds, and localities within a state. Exhibit E of the National Settlement defines core abatement strategies, as well as evidence-based and evidence-informed approved uses of settlement funding.
States and localities are not strictly bound by strategies and activities listed in Exhibit E; it serves as a useful guide for the types of activities considered to fall within the scope of “opioid abatement.” Core strategies listed as priorities include:
- Naloxone or other FDA-approved drugs to reverse opioid overdoses
- Medication-assisted treatment (MAT) distribution and other opioid-related treatment
- Pregnant and postpartum women
- Expanding treatment for neonatal abstinence syndrome (NAS)
- Expansion of warm hand-off programs and recovery services
- Treatment for incarcerated populations
- Prevention programs
Other Federal SUD Funding for States
A variety of other federal grant programs support treatment and recovery services for individuals with SUD, but they may be administered outside traditional Medicaid or behavioral health agencies. The following are key programs and funding streams that support treatment for specific populations or help augment state SUD treatment efforts:
- Department of Justice grants to support justice-involved populations: Several grant opportunities exist for state departments of corrections to provide treatment and reentry services to individuals who are incarcerated or reentering the community from incarceration. Because people who are incarcerated are ineligible for Medicaid coverage for most services, these grants are used in states to provide direct SUD treatment. The Residential Substance Abuse Treatment for State Prisoners Program provides funding and technical assistance to states to provide residential SUD treatment within state and local correctional facilities. States are also eligible to receive funding through the Comprehensive Opioid, Stimulant, and Substance Use Program (COSSUP), which can be used to support coordination across state public safety and behavioral health systems. Currently, COSSUP funds 14 state projects at a total of $65 million.
- SAMHSA and CMS funding for Certified Community Behavioral Health Clinics: States have an option for funding community services through Certified Community Behavioral Health Clinics (CCBHCs) models, which can either be funded through Medicaid State Plan Amendments or 1115 demonstration waivers, and have been supported through SAMHSA demonstration grants. CCBHCs provide coordinated, comprehensive behavioral health care to anyone who requests care for mental health or substance use, regardless of their ability to pay, place of residence, or age. The CCBHC model offers sustainable financing for a comprehensive range of services, including evidence-based treatment, care coordination, and addressing social determinants of health, by integrating care for co-occurring mental health and substance use disorders in a single setting. CCBHCs are required to provide a comprehensive set of services that include risk assessment, mental health and substance use treatment, case management, psychiatric rehabilitation services, case management, peer and family supports, 24-hour crisis management, care coordination, primary screening, and other services.
- The Centers for Disease Control and Prevention (CDC) Overdose Data to Action in States (OD2A): CDC funds 49 state health departments and Washington, DC, through a cooperative to enhance drug overdose surveillance and prevention efforts. Surveillance initiatives aim to track overdose occurrences, emerging drug threats, associated risk factors, and improve data linkage. State prevention efforts funded by OD2A grants can include harm reduction and efforts to support linkage to treatment in community settings.
- Administration for Children and Families’ Title IV-E Prevention Program: The Family First Prevention Services Act provides funding, administered by state child protection/child welfare agencies, for treatment supports to parents with SUD. These funds are intended to bolster coordinated federal and state treatment and social services funding. The act allows for the use of Title IV-E dollars to provide behavioral health prevention and treatment services to parents of children at risk of entering the state foster care system. Services delivered using this federal funding must be trauma informed and meet criteria demonstrating that they are “promising, supported, or well-supported” practices. Title IV-E is the program of last resort and not available for services payable under Medicaid to eligible parents. Federal agencies are encouraging coordination across state systems that administer these programs to take advantage of Medicaid matching as well as foster care dollars.
Acknowledgments
This report is an update of a NASHP report originally developed in 2022 by Jodi Manz and Kitty Purrington, revised by Rebekah Falkner with input from Katie Greene, Elaine Chhean, Heather Smith, and Laura Galbreath. NASHP would like to thank the Foundation for Opioid Response Efforts for its continued support in NASHP’s ongoing work to assist state leaders in opioid settlement spending and planning.


