Data Source/Resources Needed
A hospital-specific Medicare Cost Report (MCR) is the only source of information needed to complete the National Academy for State Health Policy’s (NASHP) Hospital Cost Calculator.
All Medicare-certified hospitals are required to file an annual MCR, using the Centers for Medicare & Medicaid (CMS) 2552-10 format, comprised of a series of worksheets and schedules that describe a hospital’s characteristics, financial information, staffing detail, costs, and charges.
To gain access to a hospital’s MCR, there are four possible options:
- States may require hospitals to submit their MCRs to a state agency. Each state is different, so an inquiry with the specific agency that oversees hospital reporting will confirm if the MCR is filed with the state and if public access to the report is permitted.
- Individual hospital MCRs may be requested from Medicare administrative contractors via the Freedom of Information Act (FOIA). For more information on this process, visit the CMS FOIA page.
- CMS maintains MCR data in the Healthcare Provider Cost Reporting Information System (HCRIS), which is the only government national database available for all types of hospitals (nonprofit, for-profit, and government). Downloading data in SAS dataset format is available from the CMS website.
- Private businesses have also developed databases to house the HCRIS data, format MCRs, and provide analytics. A subscription fee is required, and fees vary depending on access levels requested (e.g., a single hospital report or all hospital reports).
NASHP's Hospital Cost Tool
See NASHP’s updated interactive Hospital Cost Tool, released in February 2026.
Why Use the Medicare Cost Report?
Medicare-certified facilities are required to submit an MCR, with information such as facility characteristics, utilization data, cost and charges, and financial statement data. Facilities must complete and file a cost report on a yearly basis, due five months after its fiscal year ends. NASHP’s Hospital Cost Calculator (HCC) is designed for hospital reporting only, using CMS 2552-10 format.
The Medicare Payment Advisory Commission (MedPAC) is a non-partisan commission of 17 health care economists who annually examine and independently report to Congress on Medicare payment adequacy. The commission considers the relationship of Medicare payment to hospitals’ costs for both average and relatively efficient hospitals. The MedPAC March 2023 Report to Congress reported inpatient prospective payment systems (IPPS) hospitals’ operating margins for 2021 increased to a record high of 8.7 percent. Medicare program reimbursements to IPPS hospitals resulted in a 1 percent median margin for efficient hospitals and -6.2 percent median margin for all hospitals, including relief funds. The report also revealed not-for-profit hospitals experienced a median -8.2 percent margin, while for-profit hospitals experienced a positive 5.3 percent margin, including relief funds.
Critics of the MCR often argue that MCR reports disallow appropriate costs for the hospital. The rules rely on the basic definition of allowable costs set in federal code, 42 CFR 413.9(c)(3). Only operating costs related to hospital patient care are reimbursable under the program. Furthermore, if operating costs include amounts for luxury items or services — more expensive than those generally considered necessary for the provision of needed health services — such amounts are not allowed.
The MCR instructions summarize disallowed operating cost adjustments as follows:
- Those needed to adjust costs to reflect actual costs incurred
- Items that constitute recovery of expenses through sales, charges, fees, etc.
- Items needed to adjust costs in accordance with the Medicare principles of reimbursement
- Items that are provided separately in the cost apportionment process
The largest disallowed cost may be physician costs, and the MCR places physician costs in one of three buckets:
- Non-reimbursable services: (Medicare Disallowed) Research is the most common component, as these services do not provide patient care and are usually reimbursed through other funding.
- Professional services to individual patients: (Medicare Disallowed) Professional service reimbursement is provided through other channels, such as resource-based relative value scale (RBRVS), Medicaid/Medicare fee schedules, and commercial network agreements, etc.
- Provider services that benefit hospital patients in general: (Medicare Allowed) General services may include emergency room, intensive care unit, and other areas of general care that are not reimbursed through another channel.
To address concerns of disallowed costs, the NASHP calculator considers the full spectrum of hospital expenses. First, the calculator generates hospital breakeven points for commercial payments to cover commercial patient operating costs and any balance from government programs, charity care, care for the uninsured and bad debt. The calculator then includes more breakeven points to consider, which include Medicare disallowed costs and hospital non-operating income and expenses.
How to Fill Out the Hospital Cost Calculator
Version 4.0 calculator’s Excel workbook has eight tabs. Cells requiring data entry are shaded green, with the MCR references to the right of the cell.
Tab #1 State Government
The purpose of this tab is to present an overview of hospital financial performance, as reported in the MCR, for state government agencies and decision-makers to use as a resource.
- Sections 1–3: Financial metrics are presented by payer classification:
- Government programs (Medicare, Medicaid, SCHIP, and other low-income government programs)
- Charity care, uninsured and bad debt patients
- Medicare Advantage
- Commercial (commercial insurers, employer self-funded plans, federal employee health plan, Veterans Administration, self-pay, TriCare, and other private insurance)
- Sections 4–5: Additional financial and operating metrics are summarized from the HCC calculations and further defined in the NASHP HCT Data Variable Definitions.
- Section 6: Commercial breakeven levels present the payment levels from commercial payers that would be required for hospital revenues to cover hospital expenses with no profit. Three scenarios are presented to show hospital breakeven points. Allowance for hospital profit margin is in addition to the amounts calculated for breakeven. The references below mirror the calculator’s reporting data.
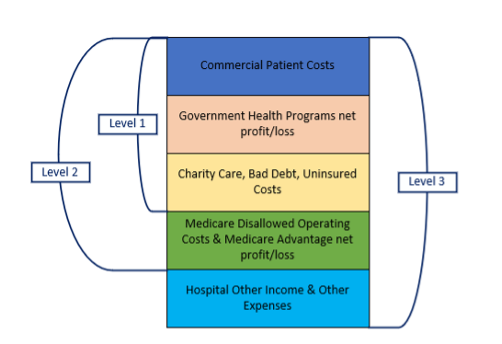
- Level 1 calculates commercial net patient revenue required to cover commercial hospital operating costs and government program, charity care, uninsured and bad debt operating profit (loss), expressed as a multiple of Medicare rate for the specific hospital.
- Level 2 calculates commercial net patient revenue required to cover Level 1, plus Medicare disallowed costs and Medicare advantage operating profit (loss), expressed as a multiple of Medicare rate for the specific hospital.
- Level 3 calculates commercial net patient revenue required to cover Levels 1 and 2, plus hospital other income and expense, expressed as a multiple of Medicare rate for the specific hospital.
- Supplemental Information. Physician-direct professional services and physician private office costs are not included in Levels 1, 2, and 3 breakeven calculations, as these costs are reimbursed through other payment channels external to hospital reimbursements (RBRVS, fee schedules, etc.). The supplemental calculation includes these costs to calculate a breakeven with their inclusion if the hospital included these expenses in the submitted MCR. Required revenue is expressed as a multiple of Medicare rate for the specific hospital.
Tab #2 Health Plan
The purpose of this tab is to serve as a resource for employer health plans by providing hospital inpatient and outpatient breakeven points to use in managing plan costs or negotiating with third-party administrators (TPAs), insurance carriers, or directly with hospitals.
- Section 1: The MCR provides the inpatient and outpatient split for Medicare patient utilization only. This Medicare split was applied to Medicaid, SCHIP and other government low-income programs, charity care, uninsured and bad debt, and Medicare Advantage patient care. The inpatient and outpatient split for commercial is calculated using the remaining inpatient and outpatient charges and operating costs.
- Section 2: Commercial Breakeven Level 3 is calculated for inpatient, outpatient, and blended inpatient and outpatient. Blended inpatient and outpatient breakeven will tie to Level 3 breakeven calculated on the State Government tab.
Tab #3 Medicare Data Entry
To alleviate confusion between the MCR and the calculator’s fields, the references will note MCR for the Medicare Cost Report and will note the HCC for NASHP’s Hospital Cost Calculator. HCC cells requiring data entry are shaded in green, with the MCR reference to the right, identifying the specific MCR worksheet location for the data. For example, “Net Assets” entry is found on Worksheet G-1, sum of columns 2, 4, 6, and 8 entries, on Line 19.
| Financial Statement Items | Amount | Source (Medicare Cost Report) |
| Fund Balance | $50,000,000 | Worksheet G-1, Columns 2, 4, 6, 8, Line 19 |
Tab #4 Medicaid and Other Data Entry
MCR Worksheet S-10; S-10, Part I; and S-10, Part II include all data points to complete Tab 4. The hospital is required to complete this worksheet, including CMS and state supplemental payments, donations for charity care, accurate calculation of uncompensated care at cost (not charges), and reporting for uninsured and bad debts.
Tab #5 Payer Mix Calculations
The purpose of this HCC worksheet is to capture hospital charge information and perform calculations required for the payer classifications:
- Medicare
- Medicaid
- SCHIP and other low-income government programs
- Charity care
- Uninsured and bad debt
- Medicare Advantage
- Commercial
Tab #6 Additional Data:
The purpose of the Additional Data tab is to capture MCR information required for calculations presented in the Hospital Cost Tool.
- Section 1: Data are entered from the various MCR worksheets.
- Sections 2–7: Calculations required for reporting metrics.
- Section 8: Reconciliations, noting all yellowed cells should equal zero. If the cell is not zero, there is a data entry error.
Tab #7 Labor:
The purpose of the Labor tab is to calculate labor metrics related to four categories: direct patient care; overhead; management and administrative; and home office and affiliates.
- Sections 1–3: Data is entered from Worksheet S3.
- Sections 4–6: Calculations required to support various labor metrics related to full-time equivalent (FTE) counts, hospital operating costs, net patient revenue, adjusted discharges, and allocations of hospital operating labor costs.
- Section 7: Reconciliation, noting yellowed cell must equal zero. If the cell is not zero, there is a data entry error.
Tab #8 Capital, Funds, Expense Allocation:
The purpose of this tab is to capture miscellaneous data related to hospital assets, capital expenses, financial investments, and expense allocation.
- Section 1: Data are entered to capture fund balance activity.
- Sections 2: Capital-related items are presented in three parts:
- Capital items reported on the hospital’s books, calculated for cost basis, and depreciated book value
- Capital assets that “relate” to the hospital, which includes assets on the books of home office or affiliates that relate to the hospital’s services, offset by assets on the hospital’s books but allocated to home office or affiliates.
- Capital-related expenses recorded by the hospital, including insurance, depreciation and amortization, interest expense, lease, taxes, and other capital-related costs
- Section 3: End-of-year cash and investments balance. For hospitals owned by a health system, it is common for the health system to hold the investments for their hospitals and other owned entities that will not be reported in the hospital’s books.
- Section 4: Hospitals are required to report revenue from sale of drugs to those other than patients.
- Sections 5–6: Hospital expenses (inclusive of all services) includes hospital reported operating expenses plus net expense increase to adjust expenses in accordance with Medicare principles of reimbursement and allowed expenses paid by home office and/or affiliates. Dollar values and percentage allocation metrics are presented for the separate components of hospital expenses (inclusive of all services):
- Direct patient care labor cost
- Labor cost other than direct patient care labor
- Capital related costs
- Other hospital operating costs
- Additional hospital expenses not related to hospital patient care