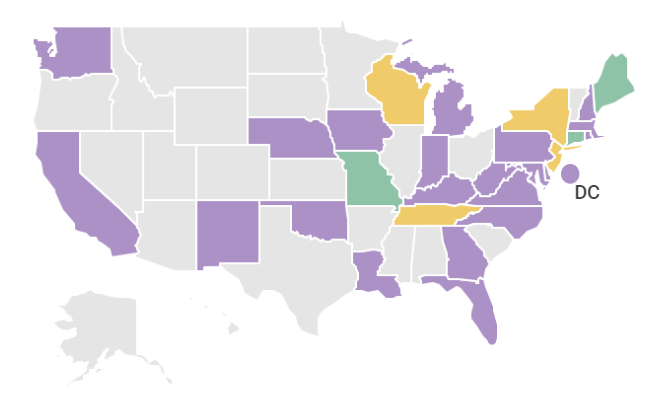
See state legislative action focused on health care payment and delivery system transformation using the map and chart below. Use the drop down menu to select the type of legislation you’re interested in. You can also see a snapshot of 2023 legislative efforts here. With questions or information about new bills, please email Allison McDowell.